Overview
Two Paths to a Fuller, More Sculpted Silhouette
Buttock augmentation has evolved considerably over the past two decades. What was once a single-technique procedure has expanded into a thoughtful menu of approaches — each suited to a different patient, a different anatomy, and a different aesthetic goal. At Dr. Newman's Beverly Hills practice, the conversation about augmentation begins not with which procedure you have heard of, but with what your body offers and what outcome you are genuinely seeking.
There are two primary surgical approaches: fat transfer — commonly called the Brazilian Butt Lift, or BBL — and silicone implants. Each has distinct advantages, distinct recovery demands, and distinct ideal candidates. Many patients arrive already committed to one option; Dr. Newman's role is to ensure that commitment is based on sound information about their specific anatomy, not simply on what is currently popular. In some cases, the two approaches can even be combined — an implant for volume alongside a modest fat transfer for contouring and shape refinement.
The Brazilian Butt Lift: Your Own Fat, Artfully Placed
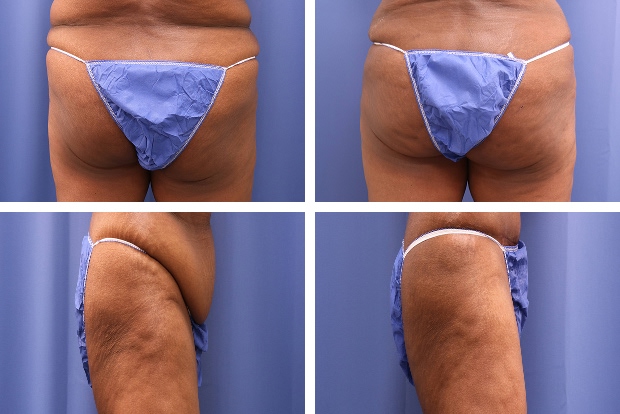
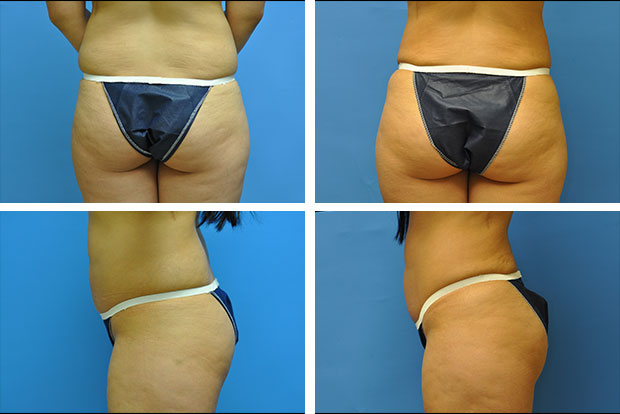
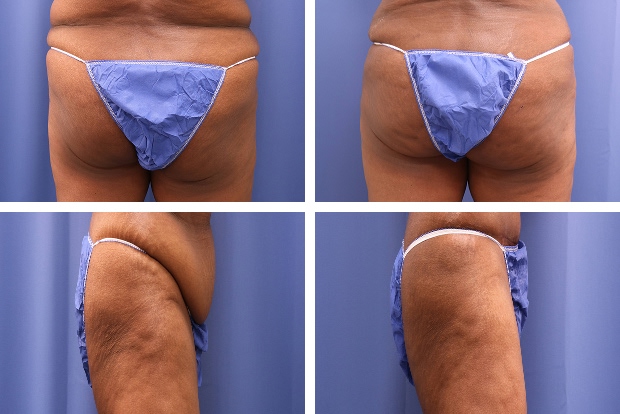
The Brazilian Butt Lift is a two-stage procedure: liposuction to harvest fat from donor areas of the body, followed by careful processing and reinjection of that fat into the buttocks. The elegance of the BBL lies in its dual benefit — the donor areas (typically the abdomen, flanks, lower back, and inner thighs) are contoured and refined by the liposuction, while the buttocks gain natural volume and improved shape. The net result is a transformation of the entire posterior silhouette: a smaller, more defined waist alongside a fuller, more projected buttock.
Fat transfer is preferred over implants whenever sufficient donor fat is available. The result feels genuinely natural — because it is your own tissue, with its own blood supply, integrated into the body. There is no foreign material, no implant-related risk of capsular contracture, and no future monitoring or replacement timeline. The fat that successfully establishes itself in the new location behaves like any other fat in the body: it responds to weight changes, feels soft and natural to the touch, and ages organically with you.
Not all transferred fat survives the procedure. The expected retention rate is typically 60 to 80 percent of what is transferred — a factor that Dr. Newman accounts for in his injection volumes. The final result becomes apparent at approximately three to six months, once the body has metabolized the fat that did not integrate and the retained fat has stabilized.
Butt Implants: A Reliable Foundation for Patients Who Need It
For patients who lack sufficient donor fat for a meaningful transfer — those who are naturally lean, have very little subcutaneous fat, or have already undergone multiple liposuction procedures — silicone butt implants offer a predictable, durable alternative. Butt implants are made from a semi-solid, cohesive silicone formulation distinctly different from breast implants: denser and more resilient to withstand the mechanical demands of the gluteal region — constant pressure, weight-bearing, and movement.
Implants are placed either within the gluteus maximus muscle (the intramuscular position) or beneath it. The intramuscular position provides natural coverage of the implant, reduces palpability, and offers the most natural appearance and feel. The surgery is performed under general anesthesia through a single discreet incision in the intergluteal crease — the natural fold between the buttocks — which heals well and is not visible in normal dress or swimwear.
The trade-off with implants is a longer, more demanding recovery than fat transfer. Because the implants are positioned within or beneath active muscle, patients may experience greater postoperative discomfort and are restricted from prolonged sitting for a longer period. Dr. Newman discusses these trade-offs candidly so that patients make this decision with full understanding of what the recovery requires.
A Note on Safety
The Brazilian Butt Lift has historically carried a higher surgical mortality rate than most cosmetic procedures — not because fat transfer is inherently dangerous, but because the specific complication it is associated with (fat embolism from intravascular injection) is largely preventable with proper technique. Fat must be deposited in the subcutaneous layer or the superficial muscle — never deep into the vascular spaces within the muscle. Dr. Newman follows the evidence-based safety protocols established by plastic surgery's leading societies: blunt-tip cannulas, controlled retrograde injection, and strict attention to injection depth throughout the procedure. Choosing a board-certified plastic surgeon with specific training in this technique is the single most important safety decision a patient can make.