Overview
Shape and Position, Restored
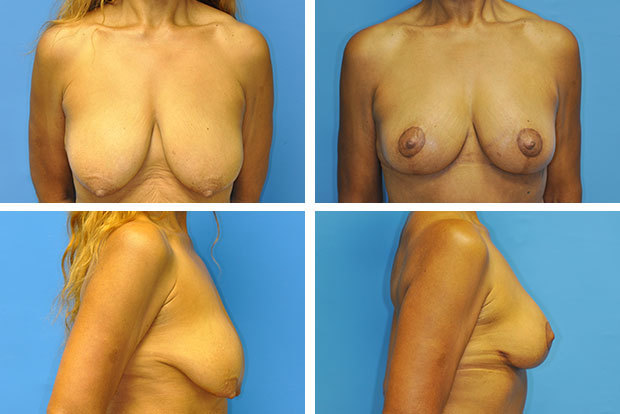
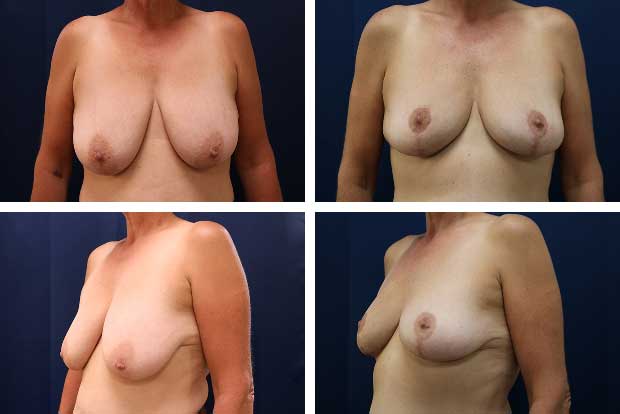
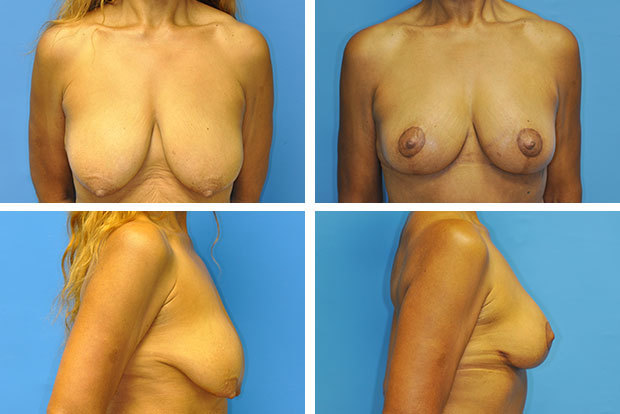
There are changes that no amount of exercise can undo. When the breast loses its position on the chest wall — the nipple descending below the breast fold, the skin stretching, the youthful roundness giving way to elongation — the problem is structural, not muscular. A breast lift, or mastopexy, addresses these changes surgically: reshaping the breast, elevating the tissue, repositioning the nipple, and removing the excess skin that is preventing the breast from maintaining its form.
It is important to understand what a lift does and does not do. Mastopexy is a procedure about shape and position, not size. It does not add volume. Most women who have a breast lift find that their breasts look very similar in size before and after — perhaps slightly fuller in the upper pole due to the more compact, elevated position of the tissue — but the dramatic transformation is in how the breast sits on the chest wall. A breast that previously drooped significantly can be restored to a position that looks and feels decades younger.
If volume restoration is also a goal — if the breasts have become not only ptotic but also deflated, often as a result of pregnancy and breastfeeding — Dr. Newman may recommend an augmentation mastopexy: a combined procedure that lifts and reshapes while simultaneously restoring fullness through implants or fat transfer. This combination is among the most commonly requested procedures in his practice, and it allows for both concerns to be addressed in a single surgery with a single recovery period.
Understanding Ptosis: Grades and What They Mean
Breast ptosis — the medical term for sagging — is classified by the position of the nipple relative to the breast fold (inframammary crease). This classification directly guides the surgical approach. Grade I ptosis (mild) places the nipple at or near the fold. Grade II (moderate) places the nipple below the fold but still pointing forward. Grade III (severe) places the nipple well below the fold, often pointing downward. Pseudoptosis describes a situation where the nipple position is acceptable but the lower breast tissue has descended, creating an empty, deflated lower pole — a pattern commonly seen after significant volume loss.
The degree of ptosis, along with the size and overall anatomy of the breast, determines which incision pattern will produce the best result for a given patient. This is not a one-size-fits-all decision, and Dr. Newman takes it seriously.
What Causes Breast Sagging?
Breast ptosis results from the gradual breakdown of several structural systems that support the breast. The skin envelope is the most visible factor — as the skin stretches and loses elasticity, it can no longer hold the breast tissue in its original position. The supportive ligaments within the breast (Cooper's ligaments) also stretch over time. Pregnancy and breastfeeding cause the most rapid and dramatic changes: the breast tissue enlarges significantly under hormonal influence, stretches the skin, and then involutes after weaning — leaving a deflated breast in an already-stretched envelope. Significant weight fluctuations produce a similar dynamic. Gravity acts continuously over years, and genetics determine how quickly and how much any individual's breast will respond to these forces.
Quick Facts
Recovery
Desk work in 1–2 weeks; full activity at 4–6 weeks
Bra
Surgical bra worn for 6 weeks post-op
Anesthesia
General anesthesia
Duration
2–3 hours
Scars
Fade significantly over 12–18 months
Size Change
Minimal — lift improves shape, not volume
Facility
Accredited outpatient surgical center
Schedule a Consultation